

Advancing Multiple Myeloma Care

Mass spectrometry (MS) is highly sensitive and specific in identifying molecules based on mass-to-charge ratio. This technology has a plethora of successful clinical applications from toxicology to microbiology. Recently, MS has been employed in multiple myeloma (MM) to assess treatment response as it is highly sensitive in measuring myeloma proteins (M-proteins) compared to available methods such as serum immunofixation electrophoresis.
The concept of MRD, a measure of residual cancer cells or their products, has been influential for other blood cancers, such as acute lymphoblastic leukemia and chronic myeloid leukemia, where it is increasingly used as a predictive biomarker to guide treatment decisions.1 The advent of more sensitive techniques for disease detection in MM has led to the expansion of MRD testing, founded on the premise that MRD-negativity is a clinically valid surrogate biomarker for progression-free survival and overall survival. Recently, the US Food and Drug Administration’s Oncologic Drug Advisory Committee voted to support using MRD as a surrogate endpoint for accelerated drug approval in MM. Myeloma Canada has also endorsed access to MRD testing to help guide the management of patients with MM. Standard techniques for measuring MRD in MM include flow cytometry (e.g., EuroFlow) and next-generation sequencing (NGS)(e.g., ClonoSeq). Both techniques require bone marrow samples and are costly and time-consuming—the costs for flow cytometry range from $300-400 USD; NGS costs over $2000 USD and requires a baseline sample.
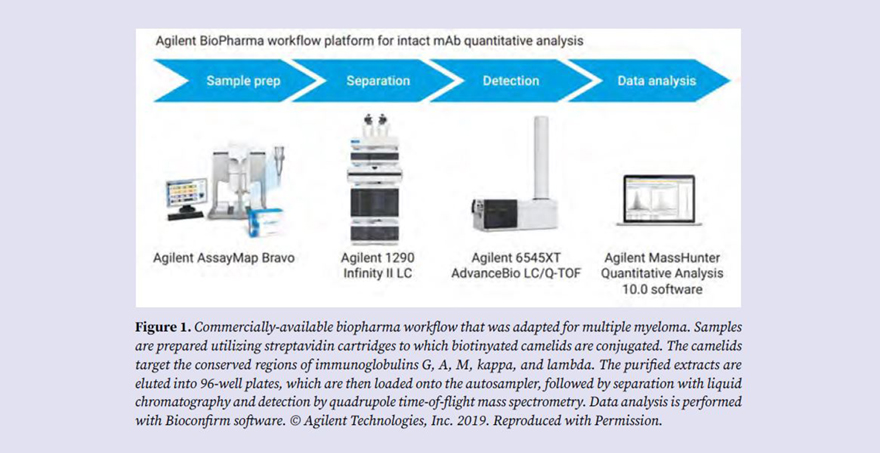
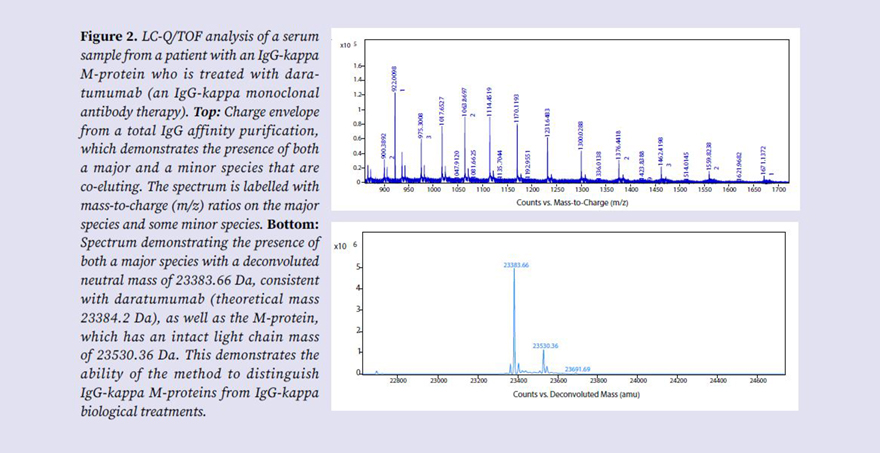
In 2021, the International Myeloma Working Group supported using MS in MM and highlighted its potential use for MRD assessment. One study comparing MS to NGS showed considerable concordance between assays ranging from 63-83%, with the best outcomes in those MS-negative alone or both MS- and NGS-negative. Discordant results have been attributed to false-negative NGS results due to spatial heterogeneity within the marrow, hemodilution of the aspirate sample, or extramedullary disease. The authors suggested that MS could be considered for MRD detection. MS in MM can be divided into intact light chain and clonotypic peptide methods. Intact light chain methods employ matrix-assisted laser desorption ionization-time-of-flight (MALDI-TOF) or liquid chromatography coupled to high-resolution mass spectrometry (LC-HRMS) such as liquid chromatography-quadrupole time-of-flight (LC-Q/TOF) MS to determine the molecular mass of intact light chain-associated M-protein above the polyclonal background. Clonotypic peptide methods identify unique M-protein peptides by sequencing, which are then monitored by LC-HRMS. Intact light chain methods also offer the advantage of differentiating therapeutic antibodies from the monoclonal proteins arising from the myeloma cells. The mass accuracy of the high-resolution LC-Q/TOF system is approximately 1 Da, which provides excellent discrimination of intact light chains based on mass. Evaluating peripheral blood samples for intact light chains is a multistep analytical process involving sample preparation by affinity purification targeting the conserved regions of immunoglobulins G, A, M, kappa, and lambda to enrich immunoglobulins and wash away unwanted serum proteins (Figure 1). Purified immunoglobulins are then separated and detected by LC-Q/TOF (Figure 2).
Access to MS testing for MM is currently limited, and commercial platforms are only just emerging. In-house developed methods have generally been restricted to select tertiary care centers and differ in cost, throughput, analytical performance, and required experience. Intact light chain methods offer significant cost and time savings and do not require sequencing as they measure the intact mass of the light chain with a single workflow. Analysis is performed on peripheral blood, allowing ease of assessment at multiple time points during the patient journey. For these reasons, intact light chain methods have generally been considered more clinically viable. MS also offers the added advantage of being able to detect post-translational modifications such as glycosylation, which have been linked to an increased risk of amyloidosis.
In our laboratory, we validated an intact light chain LC-Q/TOF method. The use of this technology in our clinical laboratory represents early adoption in Canada and opens the door to evaluating this assay for MRD assessment in our patient population. Though other MRD assays, especially NGS, remain the current gold standard, MS might offer a useful sensitive screen to determine who requires this more costly and invasive testing through a comprehensive multimodal approach for MRD evaluation. For example, if MS-negative, NGS evaluation can be considered to confirm MRD-negative status, but not if MS-positive. Future studies will be required to validate the optimal approach to MRD assessment in MM.
- Advocate - Volume 31, Issue 3, Fall 2024 (PDF, 3.06 MB)





